Sagittal split osteotomy is a surgical procedure used in orthodontics and maxillofacial surgery to reposition the lower jaw. There are various modifications of this procedure to address specific patient needs or surgical goals. Some common modifications include:
SPLIT MODS
1907: Blair described a completely horizontal osteotomy. Straight across.

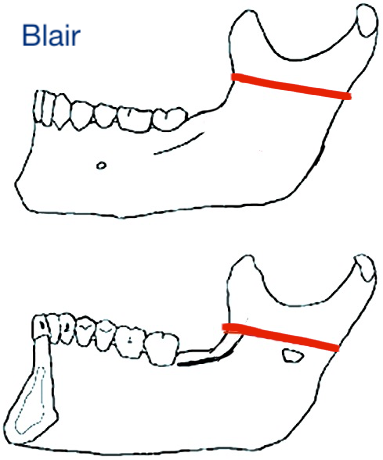
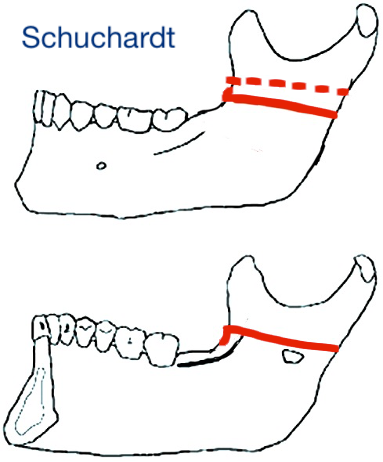
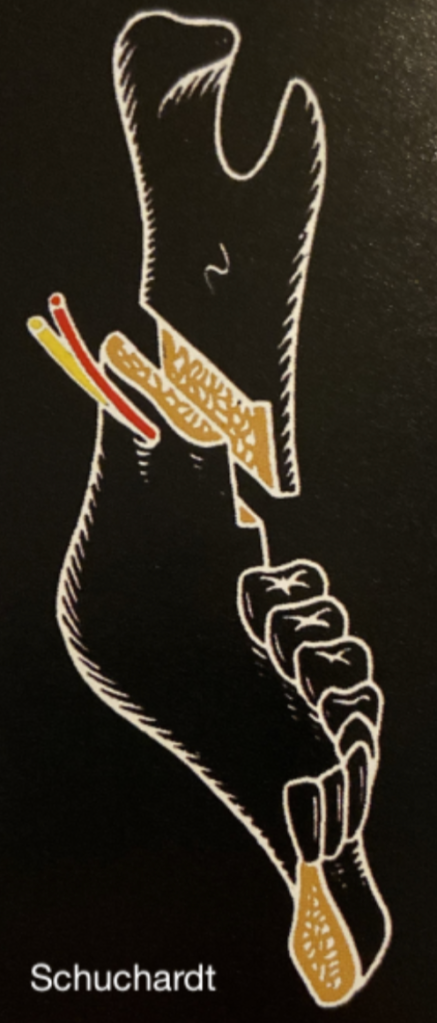
1942: Schuchardt modified the buccal osteotomy to be 10mm inferior to the lingual osteotomy; dotted line indicates Blair’s original horizontal osteotomy.
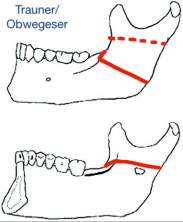
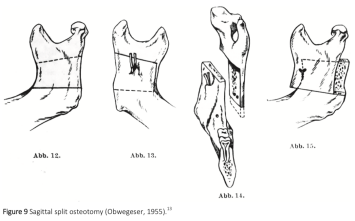
1953-1957: Trauner/Obwegeser further increased the distance between buccal and lingual osteotomies from 10mm to 25mm, thus pioneering the original sagittal split osteotomy.
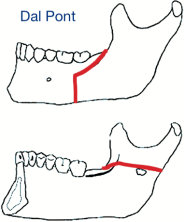
1961: Dal Pont advanced the buccal osteotomy anteriorly to the mandibular body, specifically between the 1st and 2nd molars, and turned the horizontal osteotomy into a vertical osteotomy. Note that the lingual cut extends all the way to the posterior border.
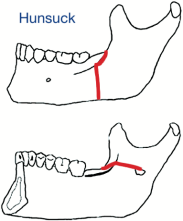
1968: Hunsuck shortened the lingual osteotomy to terminate just past the lingula. Note in all previous pictures, the lingual osteotomy extends all the way to the posterior border of the mandible. He also moved the vertical buccal osteotomy to the distal of the 2nd molar.
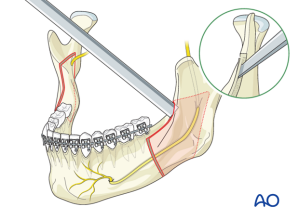
1977: Epker advocated against wide stripping of the masseter, previously thought to decrease relapse, and first suggested the need for osteotomy of the inferior border to prevent unfavorable splits.
1986: Rajchel et al., suggested the vertical osteotomy should be moved to the region of the 1st and 2nd molars, after finding the greatest distance between the neurovascular bundle and the buccal plate was in that area.
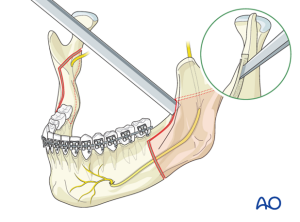
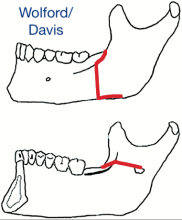
1990: Wolford/Davis introduced the concept of the inferior border split and invented a new reciprocating saw head to facilitate it (pictured below). Studies performed by Böckmann et al in 2011 confirmed the increased likelihood of a favorable split with the additional of a lingual osteotomy in animal models.
Currently, the most commonly taught and learned approach for the for BSSO include the Dal Pont, Epker, and Hunsuck modifications.
")

")